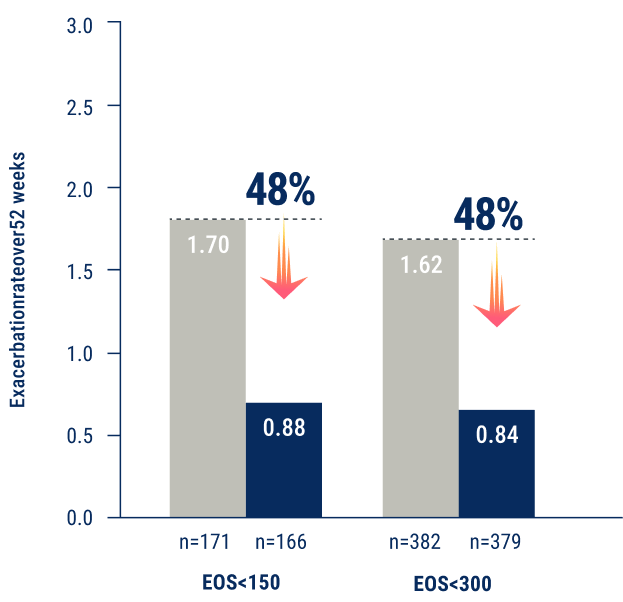
*In a pooled analysis of PATHWAY and NAVIGATOR, AAER was 0.84 for TEZSPIRE (n=379) vs 1.62 for placebo (n=382)
in patients with baseline blood eosinophils <300 cells/μL. All patients received SOC (MD or HD ICS + additional controller).22,24,25
†48% exacerbation reduction vs placebo was consistent across both the bEOS <150 cells/µL and bEOS <300 cells/µL subgroups.
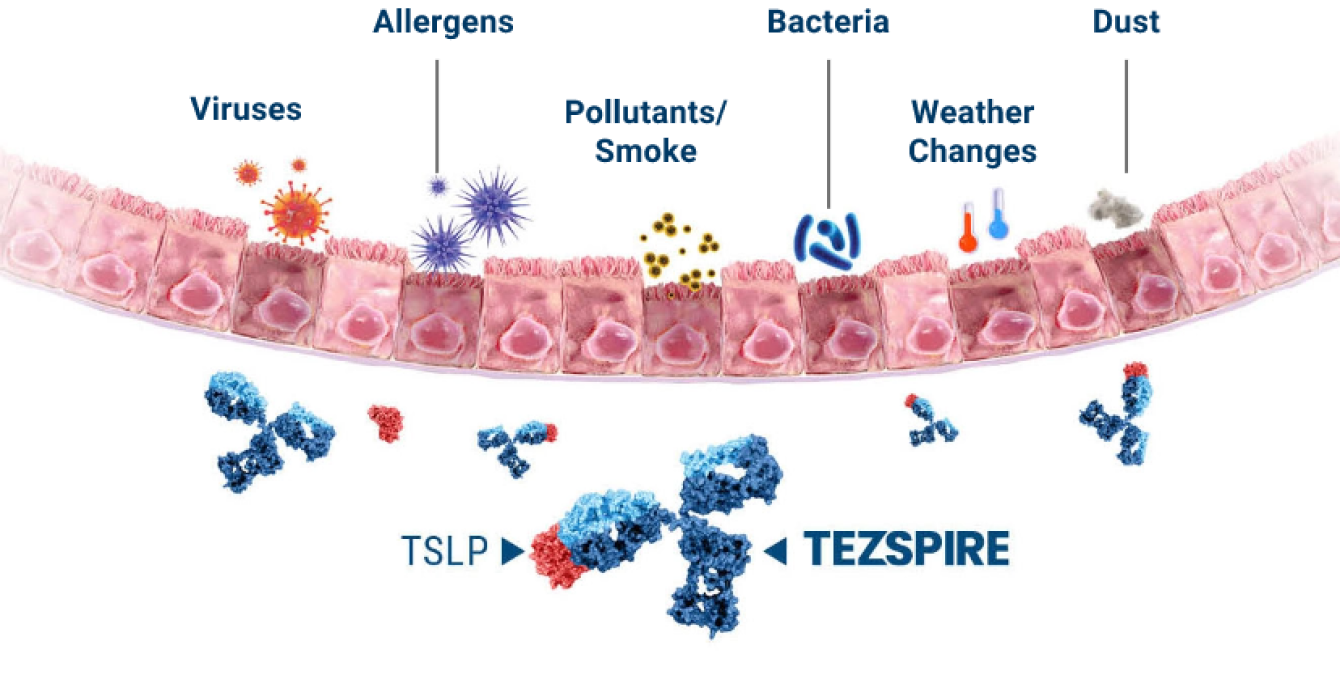
Mechanism of action
In this mechanistic study (CASCADE), airway hyperresponsiveness (AHR) to mannitol was an exploratory outcome.9
The clinical significance of this outcome and its impact on asthma have not been established.
*In the NAVIGATOR trial,5,6 patients treated with TEZSPIRE 210 mg every 4 weeks (Q4W) + SOC had least-squares (LS) mean reduction from baseline compared to placebo + SOC at week 52 in blood eosinophil counts (n=458 and n=451; -170 vs -40 cells/µL, respectively), fractional exhaled nitric oxide (FeNO) level (n=440 and n=426; -17.3 vs -3.5 ppb, respectively), and serum total IgE (n=482 and n=471; -164.4 vs +43.6 IU/mL, respectively). Results are descriptive only. In the CASCADE trial,9 the primary endpoint was the change from baseline to the end of treatment in the number of airway submucosal cells per mm2 in bronchoscopic biopsy samples. The reduction in airway submucosal eosinophils was 89% in patients treated with TEZSPIRE 210 mg Q4W + SOC (n=48) and 25% in patients treated with placebo + SOC (n=51); end of treatment to baseline geometric LS mean ratio was 0.11 vs 0.75, respectively.
‡ In CASCADE,9 AHR to mannitol was reduced in patients treated with TEZSPIRE 210 mg Q4W + SOC and placebo + SOC. There was a numerically greater reduction in AHR to mannitol in patients who received TEZSPIRE compared with those who received placebo, both in terms of absolute PD15 and in doubling doses. The clinical significance of this outcome and its impact on asthma have not been established.
CI=confidence interval; FEV1=forced expiratory volume in 1 second; IgE=immunoglobulin E; ppb=parts per billion; SOC=standard of care.
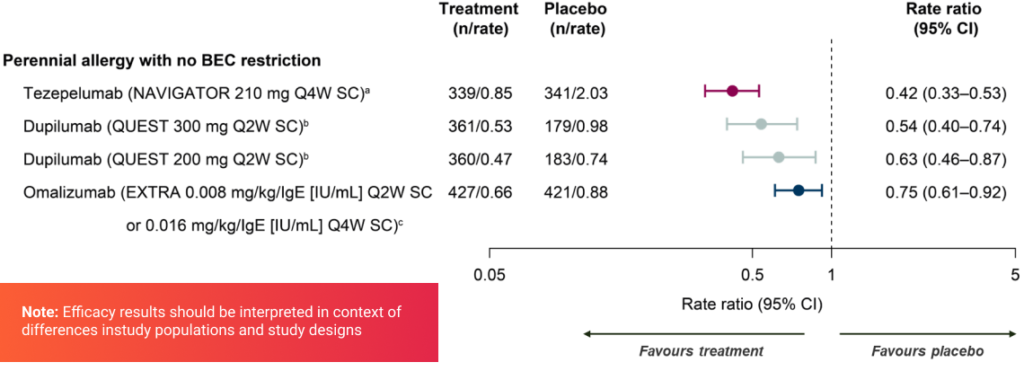
Efficacy
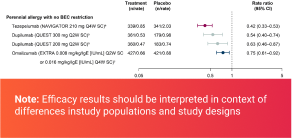
All biologics with data available reducedthe AAER in patients with perennial allergy with no BEC restriction
aRegardless of serum total IgE level; bRequired serum total IgE ≥ 30 IU/mL; cRequired serum total IgE 30–700 IU/mL
AAER, annualized asthma exacerbation rate; BEC, blood eosinophil count;CI, confidence interval; IgE, immunoglobulin E; Q2W, every 2 weeks; Q4W, every4 weeks; SC, subcutaneously
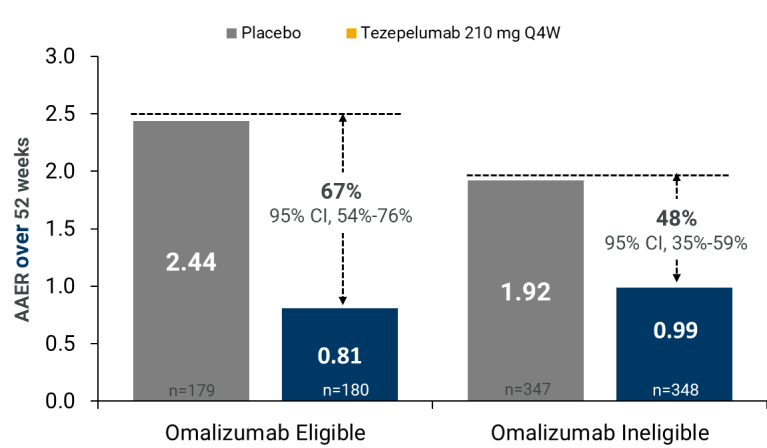
Tezspire Effect According to Eligibilityfor Omalizumab (EU definition)
Rate ratios are given with their 95% CIs. Percentage reductions relative toplacebo were calculated from rate ratios.aEligibilitycriteria were similar tothose reported in the EU label for omalizumab.2 AAER= annualized asthma exacerbation rate; ACQ-6 = Asthma Control Questionnaire-6;AQLQ(S)+12 = Standardized Asthma Quality of Life Questionnaire for 12 Years andOlder; ICS = inhaled corticosteroids; IgE = immunoglobulin E, Q4W = every 4weeks; SGRQ = St. George’s Respiratory Questionnaire.
Exacerbations Reductions across phenotypic profiles and biomarker levels
Post hoc analysis of pool ed PATHWAY and NAVIGATOR phenotype and biomarker subgroups.
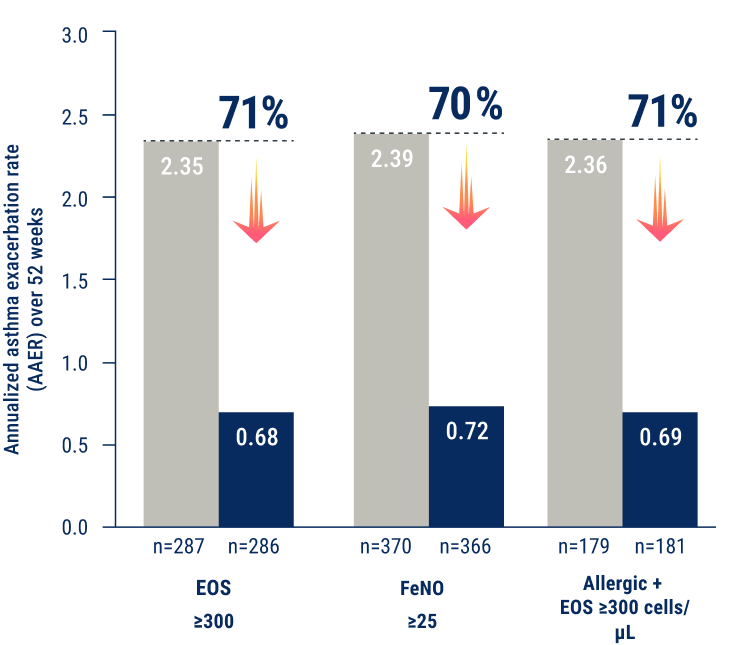
*Allergic status as defined by a serum IgE result specific to any perennial aeroallergen in the FEIA panel.
EOS=eosinophils; FEIA=fluorescence enzyme immunoassay; FeNO=fractional exhaled nitric oxide; IgE=immunoglobulin E; ppb=parts per billion; SOC=standard of care.
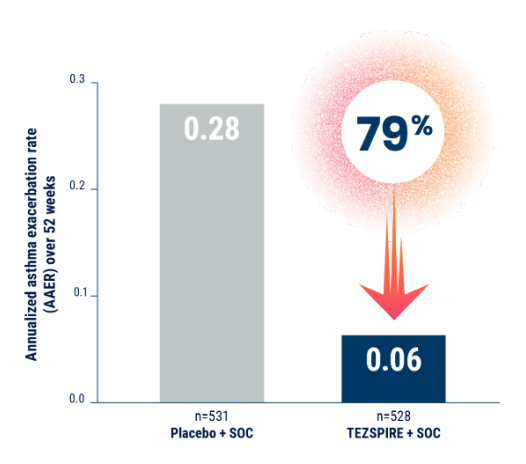
Unprecedented reductions in exacerbations – up to 71% exacerbation reduction
*PATHWAY AAER: TEZSPIRE + SOC 0.20 (n=137) vs placebo + SOC 0.72 (n=138); RR: 0.29 (95% CI: 0.16-0.51); NAVIGATOR AAER: TEZSPIRE + SOC 0.93 (n=528) vs placebo + SOC 2.10 (n=531); RR: 0.44 (95% CI: 0.37-0.53).1
†Prespecified and multiplicity-protected. Results from NAVIGATOR. TEZSPIRE + SOC AAER 1.02 (n=309) vs placebo + SOC 1.73 (n=309); RR: 0.59 (95% CI, 0.46 to 0.75; P<0.001).
AAER=annualized asthma exacerbation rate; CI=confidence interval; RR=rate ratio; SOC=standard of care.
Reduction in exacerbations requiring ED visits, urgent care, or hospitalizations
*An emergency room visit was defined as evaluation and treatment for <24 hours in an ER or urgent care center that required systemic corticosteroids.6
ED=emergency department; RR=rate ratio; SOC=standard of care.
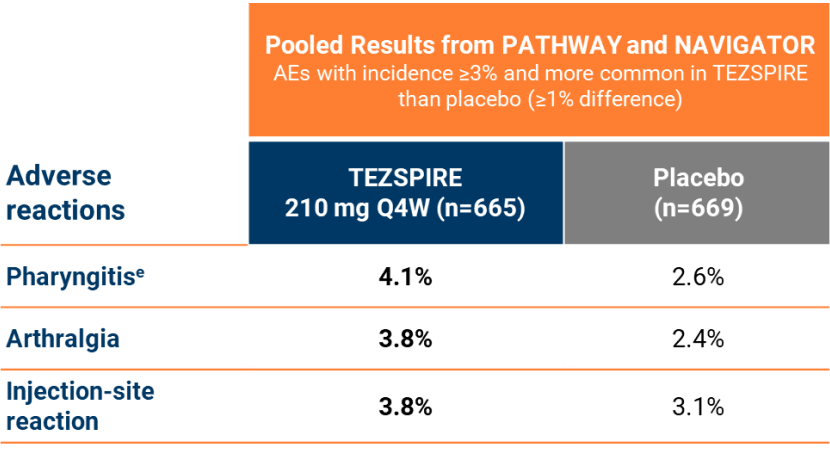
Safety PATHWAYincluded 3 tezepelumab doses; only data from the 210 mgdose are presented
aPhase IIbtrial; bPhase IIItrial; cPost-hocanalysis; dNote:Clinically relevant adverse events (rash, injection-site reaction) are alsopresented; ePharyngitis(including pharyngitis, pharyngitis bacteria, pharyngitis streptococcal andviral pharyngitis);5 fRash(including rash, rash pruritic, rash erythematous, rash macular, rash papular);4,5 gPATHWAY(N=550); NAVIGATOR (N=1059); SOURCE (N=150); CASCADE (N=116); DESTINATION(N=951; 827 from NAVIGATOR and 124 from SOURCE)
AE = Adverse Event; Q4W = Every 4 Weeks; SAE = Serious Adverse Event